Most cannabis formulations, built around just THC and CBD, can work for intimacy—but they require a certain amount of mental effort to stay in a good headspace. That’s the kind of effort you don’t need to be making.
Adding a third cannabinoid—CBN (cannabinol)—to the THC+CBD combination creates something noticeably more stable. In a 1:1:1 ratio of Δ9-THC, CBD, and CBN, the experience is self-regulating. You don’t need to steer your mood. The blend handles that, freeing your attention for your partner, your body, and the moment.
I recently tried 5-MAPB (5-(2-methylaminopropyl)benzofuran) at 80mg on a single occasion—my first experience with an MDMA-like compound. This gave me a useful point of comparison with psilomethoxin (Pm).
In my judgment, Pm at 0.5–1g most closely resembles 5-MAPB. Below that range, Pm is too subtle; above it, the experience pulls inward too firmly in a way that diverges from the 5-MAPB character.
The comparison confirmed differences I had suspected. 5-MAPB is a stimulant—sleep on the day of administration was a challenge. Pm is not a stimulant; as noted in the original case report, falling asleep at the peak is possible.
Drug regulation should not be a criminal matter, but addressed by health care providers. I urge the DEA to drop this attempt to schedule more substances.
Personal Liberty: At the heart of the decriminalization movement lies the principle of individual autonomy. Adults should have the right to choose what they put into their own bodies, as long as their actions don’t harm others. Criminalizing personal drug use infringes on this fundamental freedom, treating individuals as criminals for making private choices.
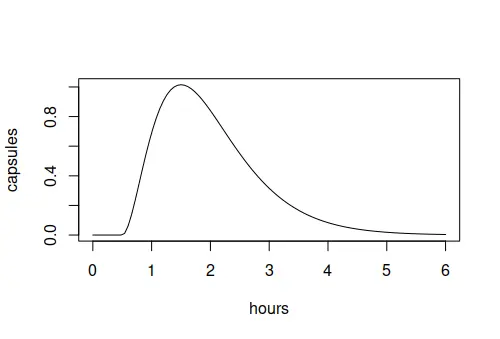
Using this function, you can estimate the effect of multiple capsules taken at different times. For example, suppose you take 2 at 10am, 1 at 10:45am, 1 at 11:15am, and 1 at 11:45am. If you space out 5 capsules like this then the peak is only about 3.5 capsules worth at 1pm:
I have had IFS sessions with one client on multiple occasions with a self-administered psycholytic dose of psilomethoxin (Pm).
In addition, I have shared Pm with five people Z, M, W, K1, and K2.
What surprised me most from this exploration is that Pm seems to have a built-in exit valve.
Or from the opposite point of view, the user only experiences the effects of Pm when focused inside.
If you focus outside then you can completely miss the effects.
For traditional psychedelics, an exit valve is an aspiration.1 For Pm, it seems already built-in!
Abstract: The use of psychedelics in therapy may benefit both the client and the facilitator, and there is a debate about whether facilitators should have personal experience with the substance. While some traditions expect the facilitator to partake in the same dose as the participants, modern medicine expects the facilitator to remain sober. Facilitator sobriety is important to attend to the risks associated with psychedelic use, while communal use of the substance may increase empathy and compassion. Further research is needed to determine the circumstances in which facilitator sobriety or communal use is appropriate.
 June 6, 2026
June 6, 2026